Every day, U.S. providers lose thousands of dollars to insurance downcoding, and most never catch it. The claim shows as “paid.” The AR dashboard looks clean. But the reimbursement is silently lower than what was earned.
Medical billing downcoding affects an estimated 8-10% of all submitted claims. Industry data shows 41% of providers now face denial rates above 10%. Yet downcoded claims rarely appear on a denial report. They hide inside remittance advice as quiet payment reductions.
Many practices simply accept the lower payment and move on. In 2026, that is the most expensive mistake a provider can make. This guide covers what insurance downcoding is, why it happens, how to detect it, and exactly how to fight back.
Insurance downcoding happens when a payer changes your submitted CPT code to a lower-level code, without issuing a formal denial. You bill CPT 99215 for a high-complexity established patient visit. The payer pays it at the rate of CPT 99213. No explanation, just a smaller check.
What makes CPT code downcoding so damaging is its invisibility. Payments arrive on schedule. Your accounts receivable (AR) looks normal. But your net collection rate quietly declines, quarter after quarter, with no visible cause.
The most frequently targeted CPT codes include:
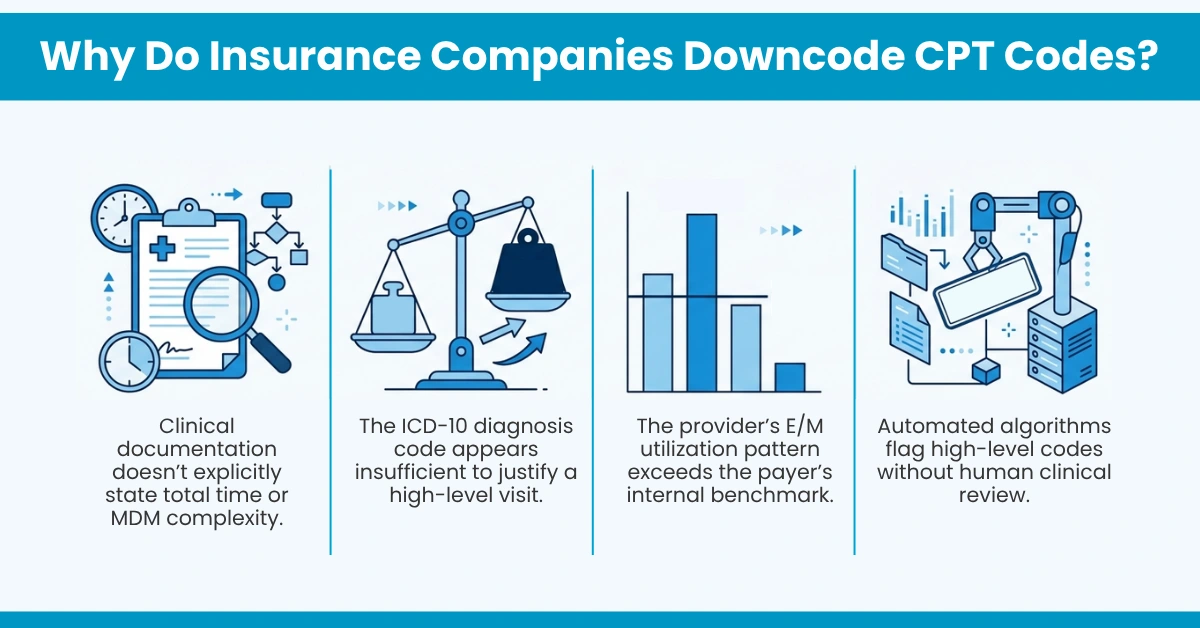
Insurers process millions of claims each year. Their review doesn’t always reflect the true complexity of a patient visit or the provider’s Medical Decision Making (MDM).
Payers increasingly rely on AI-driven editing systems that flag and downcode visits using narrow, proprietary criteria, with no human clinical review. Major payers, including Aetna, Humana, Anthem Blue Cross Blue Shield, and Cigna, have all implemented algorithmic E/M downcoding as standard practice in their adjudication systems.
Common reasons payers reduce codes:
The American Medical Association formally opposes automatic, algorithm-driven E/M downcoding without adequate clinical review. Providers have every right to challenge these reductions, especially when documentation supports the original billed code.
These two terms are frequently confused, and that confusion costs money on both sides.
Downcoding | Upcoding | |
Who does it | Payers (algorithmic) or providers (defensive) | Providers |
Financial impact | Silent revenue loss, compounding over time | Fraud risk, fines up to $23,000 per claim |
Compliance risk | Non-compliant, distorts RCM data | False Claims Act violation |
Fix | Appeal with complete documentation | Coding audit and immediate correction |
Neither is acceptable. Both require active management through a structured denial management and coding compliance workflow. Understanding this distinction protects your practice on both sides.
Most providers underestimate how fast small per-claim reductions compound into serious losses.
For a family physician managing 18-22 established patients per day, silent downcoding by Medicare Advantage plans can compound into $28,000 to $74,000 in annual revenue loss per physician. One physician-owned practice lost over $3,000 in the first half of the year from a single payer. A Missouri dermatologist lost nearly $14,000 from Anthem alone.
For multi-provider groups, these losses scale rapidly and stay invisible until a formal billing audit reveals the pattern.
The cumulative impact includes:
Even a single downgrade from CPT 99215 to 99213, across just ten visits per week, creates substantial annual revenue loss. Multiplied across a full practice, it is not a billing inconvenience. It is a financial emergency.
Most providers only discover systematic downcoding during a billing audit, months after the revenue is already gone. Proactive monitoring is the answer.
Run these checks immediately:
If a specific payer consistently pays your 99215s as 99213s, that is a programmatic policy, not a coincidence. It is fully challengeable. HelloMDs medical billing audit services are designed to catch exactly these patterns before they compound into serious losses.
The medical claim appeals process succeeds far more often than providers expect, when executed correctly.
Practices using AMA 2021 MDM documentation and payer-specific appeal templates achieve a 68% appeal overturn rate. Practices using generic letters achieve only 22%.
Follow this step-by-step process for appealing downcoded claims:
The medical record is a legal document. It is your strongest defense. According to CMS, providers are entitled to a full and fair review of all disputed claims.
Strong documentation is your best defense against CPT code downcoding before a claim ever leaves your system. Our medical billing and coding services are built specifically around this principle.
Prevention checklist for 2026:
Make downcode reviews a formal part of your revenue cycle management process, not a reactive afterthought when revenue dips.
Every downcoded claim deserves a review. Every supported claim deserves an appeal.
Accepting unnecessary downcodes means giving back revenue you already earned. Understanding insurance payer review policies, maintaining airtight clinical documentation, and challenging incorrect reductions through a structured medical claim appeals process are non-negotiable steps in protecting your practice in 2026.
At HelloMDs, our AAPC-certified team helps providers nationwide identify reimbursement opportunities, review downcoded claims, reduce denial rates, and optimize every stage of the revenue cycle, so you receive appropriate healthcare provider reimbursement for every level of care you deliver.
This content is for educational and informational purposes only. It doesn’t constitute legal, compliance, or medical billing advice. Providers should consult a certified billing professional or legal counsel before making coding, billing, or appeal decisions specific to their practice. HelloMDs services comply with all applicable federal, state, and payer regulations.