If your billing team is still submitting CPT code 99442, your claims are getting denied automatically. Many practices across the U.S. don’t realize that the AMA officially deleted CPT 99441-99443 effective January 1, 2025, and they are losing reimbursements because of it.
This guide cuts through the confusion. You will learn exactly what 99442 was, why it was removed, what codes replaced it in 2026, and how to document and bill correctly so your practice gets paid. Whether you run a small clinic or a multi-specialty group, this is the information your billing team needs right now.
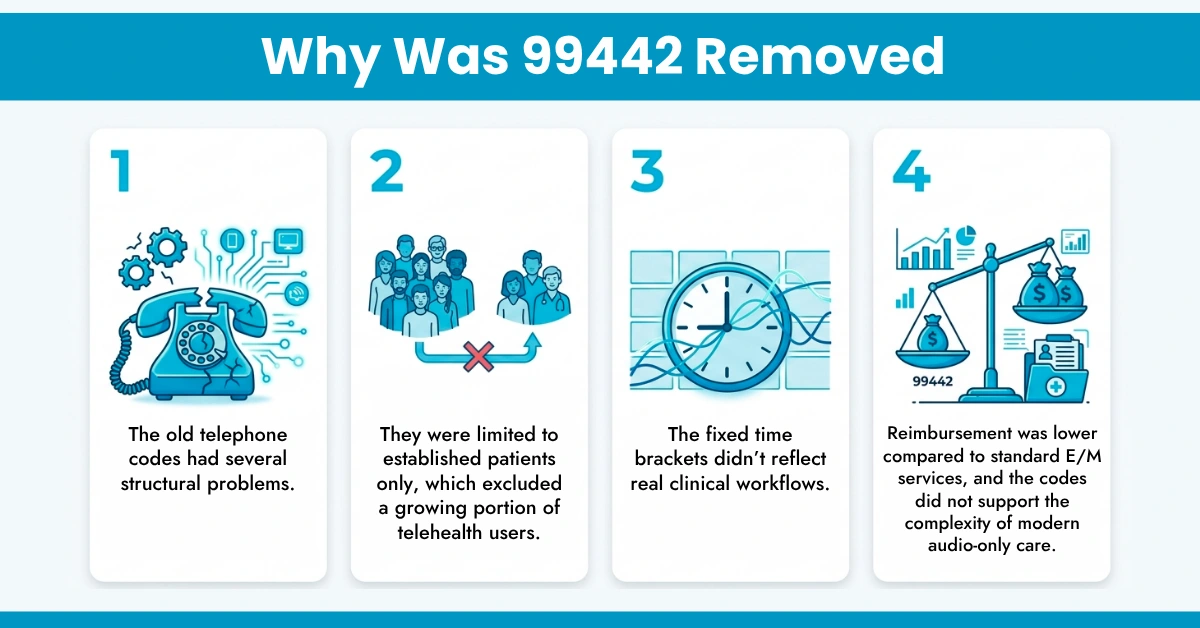
CPT 99442 describes a telephone evaluation and management (E/M) service provided by a physician or qualified healthcare professional to an established patient.
It required:
It was part of a legacy code set:
These codes are now end-dated and replaced under updated telehealth coding frameworks.
No. CPT code 99442 is permanently deleted as of January 1, 2025, and remains invalid in 2026. The American Medical Association (AMA) removed codes 99441, 99442, and 99443 from the CPT code set entirely.
Any claim submitted using 99442 in 2026 will be automatically denied by payers. This is not a temporary suspension. It is a permanent deletion.
The AMA replaced them with a more flexible, clinically accurate framework using time and MDM based audio only codes aligned with standard E/M logic.
The AMA introduced a new family of telehealth E/M codes, CPT codes 98008 through 98015, to replace the deleted telephone codes. These new codes cover synchronous audio-only evaluation and management services.
Unlike the old codes, the new ones support both time-based and Medical Decision-Making (MDM)-based selection, which aligns with standard E/M logic.
The 2026 Audio-Only Code Reference Table
New CPT Code | Patient Type | MDM Level | Minimum Time |
98012 | Established | Straightforward | 10+ minutes |
98013 | Established | Low | 20+ minutes |
98014 | Established | Moderate | 30+ minutes |
98015 | Established | High | 40+ minutes |
98008-98011 | New | Straightforward to High | 10-40+ minutes |
Here’s how to translate your 2024-2025 billing mindset into 2026 rules:
Key takeaway:
The shift from 99442 to the new 98000-series codes is more than a number change. It reflects a fundamental upgrade in how audio-only care is categorized and valued.
Three Major Differences
This is where most billing teams get confused, and it is critical to understand. The Centers for Medicare & Medicaid Services (CMS) didn’t adopt the new 98000-98015 codes for Medicare reimbursement. CMS determined these codes are duplicative of existing covered E/M services.
If you submit 98012-98015 to Medicare, those claims will be denied. HelloMDs denial management services help practices navigate exactly these payer-by-payer differences and recover revenue lost to preventable denials.
Correct coding means nothing without proper documentation. This is one of the top audit triggers for audio-only telehealth claims in 2026.
Your clinical note needs to capture:
You must also document patient consent for the audio-only service. Many payers now require a note confirming that the video was available but not used, either due to patient preference or technical limitations. Missing this can result in a denial even when the service itself was appropriate.
Audio-only codes cannot be billed alongside an in-person or audio-video E/M service for the same patient on the same day. Practices using HelloMDs coding and medical billing services benefit from certified coders who review documentation accuracy before claim submission, reducing first-pass denial rates significantly.
Even after switching from 99442 to the correct 2026 codes, billing errors still happen. These are the mistakes that cause the most denials and revenue loss.
If your practice has experienced repeated telehealth denials, HelloMDs RCM and accounts receivable services are designed to investigate root causes and rebuild a clean claim pipeline.
CPT code 99442 is gone. Practices still using it are receiving automatic denials and leaving reimbursements uncollected. The 2026 billing landscape requires a clear shift to the 98000-series audio-only codes, with the right documentation, correct payer rules, and proper modifiers.
The good news is that the new framework is more clinically accurate and, for many services, allows higher reimbursement when documented properly. Getting this right protects your revenue and keeps your practice compliant.
HelloMDs is a HIPAA-compliant, AAPC-certified medical billing company serving providers nationwide, from Texas and California to New York and Florida. If your practice needs expert support navigating 2026 telehealth billing rules, connect with our team for a free consultation.
Follow HelloMDs on Facebook and Instagram for the latest billing updates, coding tips, and RCM insights.
This article is intended solely as a professional reference to help readers understand CPT coding updates and billing practices. It doesn’t replace official payer guidelines, AMA updates, or individual clinical billing judgment. Coding rules and reimbursement policies may vary by insurer, region, and claim context, so always verify details with current payer requirements before submission. Any images or visuals included in this blog that are labeled or presented as illustrations may be AI-generated. They don’t depict real patients, providers, or clinical scenarios.