If your claims for abdominal ultrasounds keep getting denied, or you’re unsure whether to bill 76705 or 76700, you’re not alone. Thousands of billers make this mistake every week, and it costs practices real money. Worse, many providers don’t realize the 2026 Medicare fee schedule changes directly affect how much they’re reimbursed for this code.
This guide covers everything: What 76705 actually includes, which diagnosis codes support it, how diabetic patients create unique billing considerations, and how to stop leaving money on the table.
CPT 76705 describes a real-time abdominal ultrasound with image documentation, limited to a single organ, quadrant, or follow-up study. The word “limited” is doing all the legal and financial work in that definition.
Required for billing:
If either is missing, the claim is not billable under CMS rules.
This code is used across radiology, emergency medicine, gastroenterology, hepatology, and primary care, in both facility and non-facility settings.
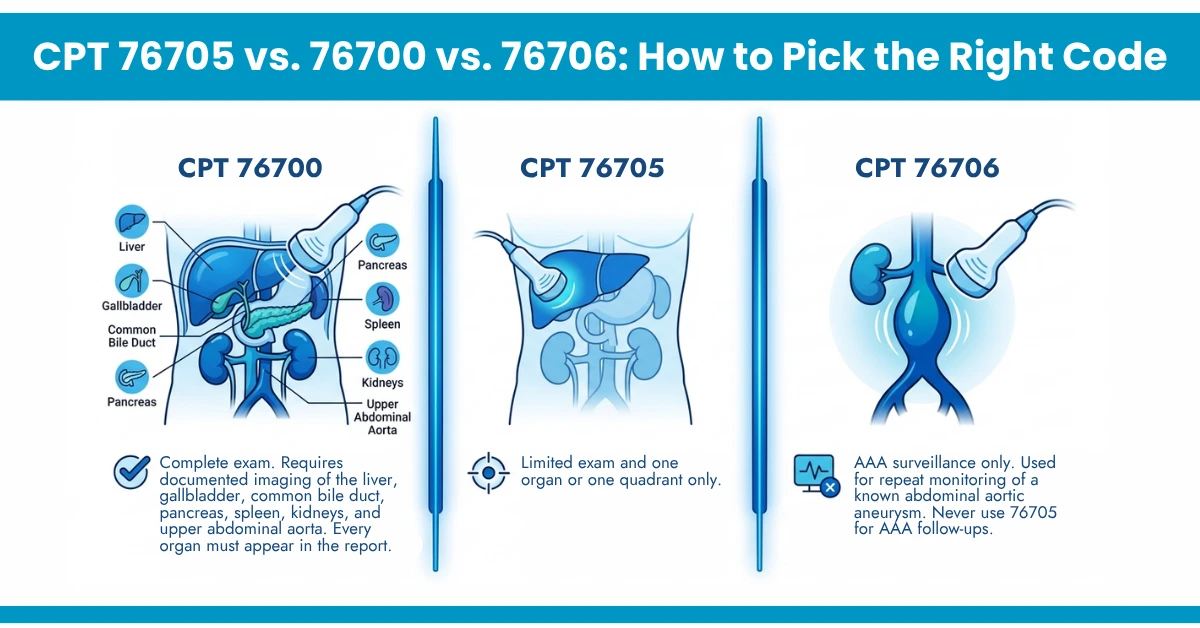
If a sonographer starts a limited scan and findings require expanding coverage mid-study, the scan may no longer qualify as 76705. If resulting images document the liver, gallbladder, pancreas, spleen, kidney, and aorta, bill 76700, not 76705. Billing the limited code for a complete exam is undercoding. It creates audit exposure in both directions.
The Down-coding risk that cut your payment:
In 2026, payers use automated auditing to detect missing organ documentation. Bill 76700 but fails to document the IVC or common bile duct, and your claim gets automatically down-coded to 76705, no notice, no explanation, just lower payment.
If an organ is surgically absent, you must state it directly in the report: “Gallbladder is surgically absent.” Silence defaults to “not examined,” which defaults to the limited code and the lower reimbursement. This single documentation line protects hundreds of dollars per claim.
ICD-10 Codes That Prove Medical Necessity for CPT 76705
The diagnosis on the claim must match the ordering provider’s documented clinical indication. Vague or mismatched codes are the single biggest driver of medical necessity denials.
Clinical Indication | ICD-10 Code | Notes |
Right upper quadrant pain | R10.11 | Most common ED billing trigger |
Acute cholecystitis | K81.0 | Gallbladder-targeted scan |
Fatty liver disease (NAFLD/MASLD) | K76.0 | Critical for diabetic patients |
Type 2 diabetes with nephropathy | E11.22 | Renal ultrasound monitoring |
Type 2 diabetes with fatty liver | E11.65 + K76.0 | Dual code proves a limited scan is needed |
Abnormal liver function tests | R74.8 | Must appear in ordering note |
Flank pain with hematuria | R10.9 + R31.9 | Kidney stone workup |
Pancreatic cyst surveillance | K86.2 | Follow-up of known cyst |
Abdominal mass | R19.09 | Quadrant-specific imaging |
Hepatomegaly | R16.0 | Liver enlargement workup |
ICD-10 codes update every Year in October 1. Using a deleted code triggers automatic rejection with no appeal path. Build a quarterly code audit into your billing workflow.
It is the most important one for internal medicine, endocrinology, and family practice billers. Patients with Type 2 diabetes (E11.x) carry an elevated risk for several abdominal conditions requiring regular targeted monitoring.
The billing error that costs endocrinology practices the most:
Placing E11. x as the primary ICD-10 when the ordering note specifies abdominal pain. Payers deny medical necessity because a diabetes diagnosis alone does not justify a limited abdominal scan. The symptoms justify it. The diabetes code supports it.
Most billing teams know a change has happened. Very few know what specifically changed and how it affects their 76705 claims. The 2026 Medicare Physician Fee Schedule (CMS-1832-F) made three changes that directly impact this code.
Modifier 26 is specifically protected: CMS confirmed identical PE RVUs in both settings for professional-component-only billing.
Most denials are preventable.
Incorrect ICD-10 Pairing: Diagnosis does not support medical necessity.
At HelloMDs, our denial management team resolves these daily, with a 99% first-pass ratio and a proven 15% denial reduction across our client practices. Our medical coding services ensure every 76705 claim leaves clean.
Use this before claim submission:
CPT code 76705 demands precision in documentation, diagnosis coding, and modifier selection. With the 2026 Medicare fee schedule cutting radiology reimbursements and payer audits becoming increasingly automated, there is no margin for errors. Practices managing high volumes of diabetic patients have the most to gain by getting this right.
If your team needs a billing partner who handles every nuance covered in this guide, HelloMDs is ready. Our AAPC-certified coders deliver a 99% first-pass ratio and a proven 15% denial reduction, nationwide.
Follow us on Facebook and Instagram and get the latest billing updates without missing anything.
This content is for educational purposes only. Always consult the current AMA CPT Manual, your local MAC, and a certified billing professional before making coding decisions. HelloMDs is not responsible for payer-specific or regional MAC variations. Pictures that you see in this content are generated from AI tools.