Most 90837 denials are not caused by fraud. They are caused by one small documentation gap, a missing start time, a vague clinical note, or a diagnosis that doesn’t match the session length on paper. CPT code 90837 is the highest-reimbursing individual psychotherapy code in mental health billing, and it is also the most audited. Payers run pattern analysis on every practice billing this code.
This guide covers the 2026 billing rules clearly: time thresholds, current Medicare rates, ICD-10 pairings that actually support medical necessity, and the top documentation mistakes auditors look for first.
The AMA defines procedure code 90837 as “Psychotherapy, 60 minutes with patient.” The official label is slightly misleading. The actual billing threshold is 53 minutes of direct, face-to-face therapeutic time, not a full 60. This is known as the CPT midpoint rule: the cutoff sits halfway between the maximum of 90834 (52 minutes) and the 60-minute benchmark.
Here is the full individual psychotherapy time ladder:
CPT Code | Session Duration |
90832 | 16-37 minutes |
90834 | 38-52 minutes |
90837 | 53 minutes or more |
The session clock runs only during active clinical engagement. It excludes scheduling, payment collection, post-session documentation, or waiting for a late patient. If the note says 50 minutes, the correct code is 90834, every single time.
A wide range of licensed clinicians can bill CPT 90837, but your license type directly affects how much you receive, a distinction most competitors skip entirely.
Medicare-eligible provider types include:
Credential level changes your actual payment in 2026. A psychologist billing 90837 receives approximately $154-$167 nationally under Medicare. An LMFT or LMHC receives approximately $115-$125. 75% of that rate. For group practices with mixed credentials, this difference matters significantly in revenue forecasting.
Before your first claim goes out, every provider must be properly enrolled with each payer. HelloMDs handles the full credentialing and enrollment process from PECOS enrollment to payer contracting, so nothing gets delayed at the credential level.
Reimbursement depends on setting, geography, and credential type. The 2026 national average Medicare rates based on the CMS Physician Fee Schedule are:
Setting | National Average |
Non-facility (private office) | ~$154-$167 |
Facility (hospital outpatient) | ~$122-$138 |
Non-facility rates are higher because the provider absorbs overhead directly. Medicare covers 80% of the approved amount; the patient owes approximately $31–$33 per session in coinsurance after meeting the Part B deductible.
Commercial payer benchmarks in 2026:
Verify your contracted rates monthly. Many underpayments result from payer system errors, not payer intent, and they rarely get corrected unless you flag them. HelloMDs provides real-time performance reports and AR follow-up that catch underpayments before they age out.
Also worth noting for eligible Medicare providers: MIPS/QPP participation in 2026 can add up to a 5% bonus on Medicare reimbursements. This is separate from your base rate and applies to providers reporting quality measures.
A correct code of selection alone does not protect a claim. The diagnosis must justify the session length. Payers flag mild or unspecified diagnoses paired with 90837 immediately.
Diagnoses that consistently support extended individual therapy:
ICD-10 Code | Description |
F32.1 | Major depressive disorder, moderate |
F33.1 | Major depressive disorder, recurrent, moderate |
F41.1 | Generalized anxiety disorder |
F43.10 | PTSD, unspecified |
F60.3 | Borderline personality disorder |
F31.30 | Bipolar disorder, depressed, unspecified |
Two accuracy points competitors consistently miss: First, severity specificity matters, F32.0 (mild depression) without documented functional impairment creates audit exposure. Second, Z-codes alone (e.g., Z63.0 for relationship distress, Z56.0 for work stress) do not justify extended psychotherapy under Medicare or most commercial payers when used without a primary mental health diagnosis.
90785 (Interactive Complexity): This add-on code can accompany 90837, but only with documented complicating factors: use of an interpreter, a legally authorized third-party present, a minor whose caregiver actively participated, or severe behavioral disruption during the session. Using 90785 without documented evidence of one of these four criteria is a direct audit trigger.
90837 vs. 90838: The Most Misunderstood Distinction in Mental Health Billing
If the entire visit is psychotherapy, only bill 90837 as a standalone code.
If psychotherapy occurs alongside separately identifiable medication management or evaluation, bill the appropriate E/M code (99213 or 99214) + 90838 (add-on).
Billing standalone 90837 alongside an E/M on the same date generates an automatic duplicate service denial. These codes work together, but only in the right configuration.
HCPCS and Telehealth Modifiers: For telehealth delivery in 2026, telehealth parity for behavioral health is permanent under Medicare. Video sessions reimburse at the same rate as in-person.
A wrong POS code is one of the most common and most preventable telehealth billing errors.
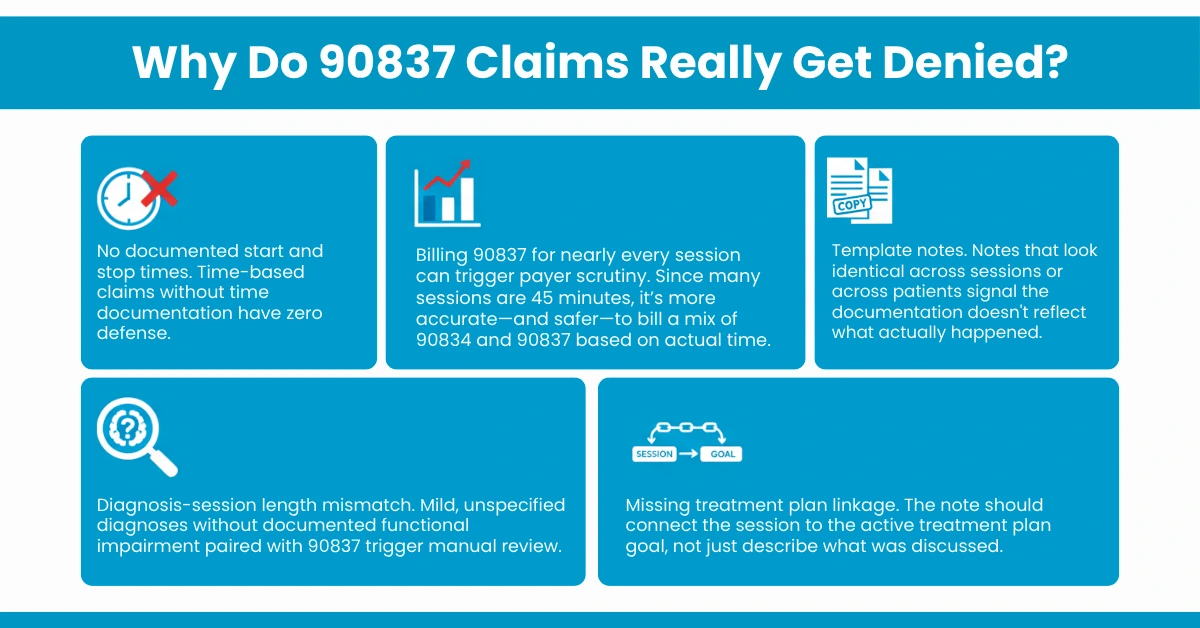
The audit patterns auditors look for first:
HelloMDs’ mental health billing team reviews claims for all five of these triggers before submission. Their denial management specialists identify root causes, time documentation, modifier errors, diagnosis mismatch, and resubmit corrected claims efficiently. Billing plans start at 2.95% of monthly collections. Contact HelloMDs for a free consultation to find out how much your current billing process may be leaving behind.
CPT code 90837 pays the highest rate for individual psychotherapy and demands the most precise documentation to protect it. In 2026, the rules are clear: document session time exactly, match your ICD-10 severity to the session length, use add-on codes only when the clinical evidence supports them, and apply the correct modifiers for telehealth. If your practice is losing revenue to denials, pattern audits, or underpayments, a dedicated billing partner like HelloMDs provides a system built to prevent it, not just fix it after the fact.
This guide provides general information on CPT code 90837 billing based on publicly available CMS, AMA, and industry sources. Coding, reimbursement, and coverage policies vary by payer, location, and provider credentials. Always verify current payer policies, document medical necessity per session, and consult licensed billing experts like HelloMDs. HelloMDs offers no legal or financial advice. The visuals shown in this blog are generated by AI tools for illustrative purposes.