Struggling with 93268 CPT code denials? Cardiology billers lose $200-400 per claim from vague ICD-10s or missing 24-hour logs. If you’re a cardiology biller, coder, or physician’s office manager and you’ve Googled “93268 CPT code description,” you’re probably dealing with one of three problems:
You’re not overthinking it. 93268 is genuinely one of the trickiest event monitoring codes to bill cleanly. This guide solves it fast with checklists, payer-proof tips and HelloMDs AAPC-certified fixes.
CPT 93268 covers an external cardiac event monitor worn by a patient for up to 30 days. It records the heart’s electrical activity either when the patient activates it due to symptoms or when the device automatically detects an abnormal rhythm.
The official description:
External, patient- and auto-activated electrocardiographic rhythm event recording with a symptom-related memory loop, remote download capability up to 30 days, 24-hour attended monitoring, including transmission, review, and physician interpretation.
Three words matter most here: 24-hour attended monitoring
CMS confirms event monitors:
Missing proof of attended monitoring = top audit failure.
Bill 93268 globally if your practice handles everything. Use components if outsourcing.
|
Code |
Covers |
Who Bills |
2026 RVU Est. |
|
93268 |
Full service: setup, recording, transmission, and physician interpretation. |
Practice that owns equipment and interprets |
1.2 Global ($247 avg) |
|
93270 |
Recording only (connection, recording, disconnection) |
Device company or technical-only provider |
0.5 tech |
|
93271 |
Transmission/analysis only |
Monitoring center |
0.4 tec |
|
93272 |
Physician review and interpretation only |
Interpreting physician only |
0.85 pro |
The rule: If your practice owns the equipment and the physician interprets the results, bill 93268 globally. If the device company does the recording and your physician only interprets, bill 93272 for your side.
Note:
Do not bill 93270 and 93271 in the same 30-day period as 93268. Payers treat 93268 as inclusive of the others. All codes in this family (93268-93272) are telemedicine codes, listed in CPT Appendix P. In 2026, audio-only temporary telehealth codes were removed. Use permanent telehealth codes with Modifier 95 and full documentation.
Vague codes are the #1 reason 93268 claims get flagged as “not medically necessary.”
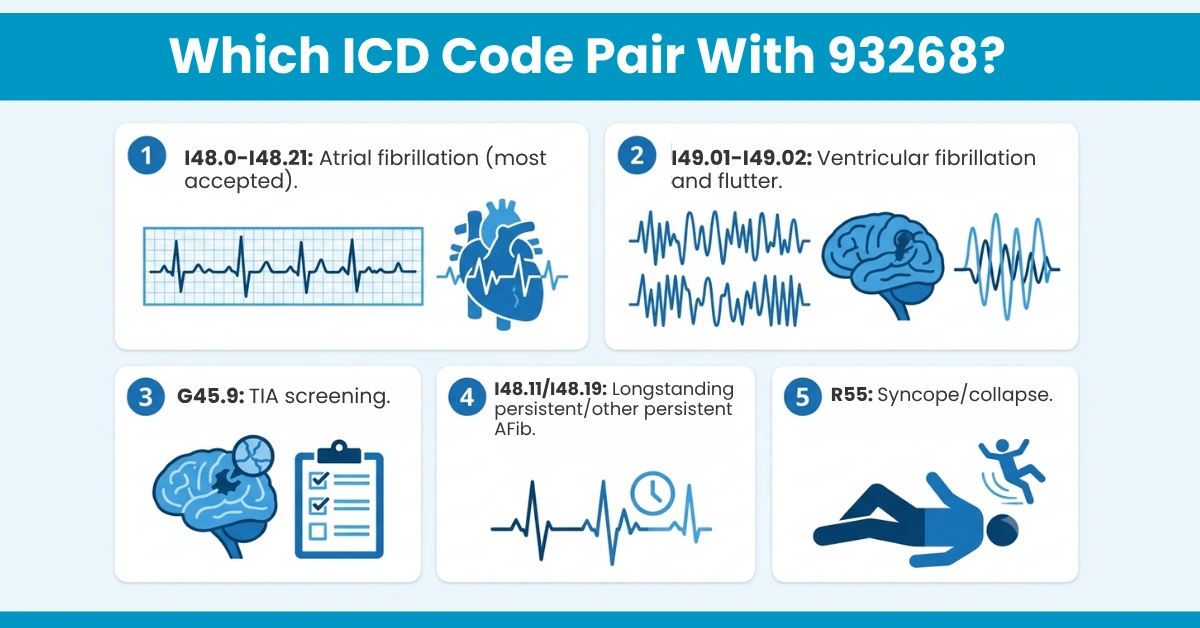
Strong Primary Diagnosis (Most accepted):
Symptoms-Based Pairings (Use them with caution):
Avoid: Using I49.9 (cardiac arrhythmia, unspecified) or I10 (hypertension) alone as your primary diagnosis. These trigger automatic medical necessity reviews at most payers.
Cigna, UnitedHealthcare, and Anthem all require documentation showing the monitoring is for presyncope, severe palpitations, post-TIA, or when Holter monitoring was inconclusive. Document that specifically in your chart notes.
Payers evaluate 3 key factors:
Missing any of these causes high denial risk
Getting modifiers wrong on 93268 is expensive. Here’s what applies:
Allowed:
Not Allowed:
Frequency watch:
UnitedHealthcare classifies 93268 as a time-span (monthly) code, with only one unit per 30-day period. Many payers, including some Medicare contractors, limit it to once every six months per patient.
Always check your specific MAC policy and payer contract before submitting.
This is where many practices lose money.
Don’t use 93268 if:
Incorrect billing risks downcodes, rejections, and audits. HelloMDs audits prevent this via cardiology billing services.
Auditors and payers look for this exact checklist. If any item is missing, the claim is vulnerable:
Note:
You need to document that the patient was instructed on device use and activation. If the device was “home-enrolled” (patient sets it up at home), document that too. It doesn’t disqualify the claim, but it must be noted.
These are the real denial patterns, pulled from actual biller communities and payer policy reviews:
At HelloMDs, our AAPC-certified coders scrub 93268 claims for exactly these patterns before they go out the door. Our denial management team and cardiology billing specialists work together, so you stop losing money to preventable rejections and spend more time on patient care.
CPT code 93268 isn’t complicated once you understand its logic: it’s a global, timespan, attended-monitoring code that requires specific clinical justification, strict documentation, and precise modifier use. The practices that get denied aren’t making big mistakes. They’re making small, preventable ones: a vague ICD-10 here, a wrong modifier there, a missing monitoring log.
If your practice is billing cardiology and you’re still chasing denials, that’s time and revenue you shouldn’t be losing.
HelloMDs serves cardiology practices across all 50 U.S. states with end-to-end medical billing and coding, denial management, accounts receivable follow-up, and credentialing services, all handled by AAPC-certified professionals. Our plans start as low as 2.95% of monthly collections.
Book your free consultation with HelloMDs today and let your billing work as hard as you do.
This article is for informational purposes only and does not constitute legal, medical, or billing advice. CPT codes, ICD-10 codes, and payer policies are updated annually. Always verify current coding guidelines with the AMA CPT Codebook, CMS, and your local Medicare Administrative Contractor (MAC) before submitting claims. Visuals in this article are generated from AI tools.