In the United States, over 10 million people are living with osteoporosis, and nearly 44 million have low bone density, putting them at increased risk for fractures. Understanding the correct ICD-10 code for osteoporosis is essential for accurate diagnosis, billing, and treatment documentation. Whether you’re a clinician, coder, billing specialist or practice manager, understanding the correct code and when to use it.
In this guide, we’ll walk you through the codes for osteoporosis unspecified ICD-10, age-related osteoporosis ICD-10, postmenopausal osteoporosis ICD-10, and screening codes like ICD-10 screening for osteoporosis.
Hello MDs’ experts fill gaps that many competitors miss, integrate practical examples tied to real practice workflows, and ensure you leave with clear, actionable knowledge.
A common question among healthcare professionals is: what ICD-10 code should be used for osteoporosis? The answer depends on two key factors:
The main categories in the US version of the classification are:
Understanding ICD-10 coding for osteoporosis is just one part of effective chronic disease billing. Learn how similar coding applies to metabolic disorders in our post on Dyslipidemia ICD-10.
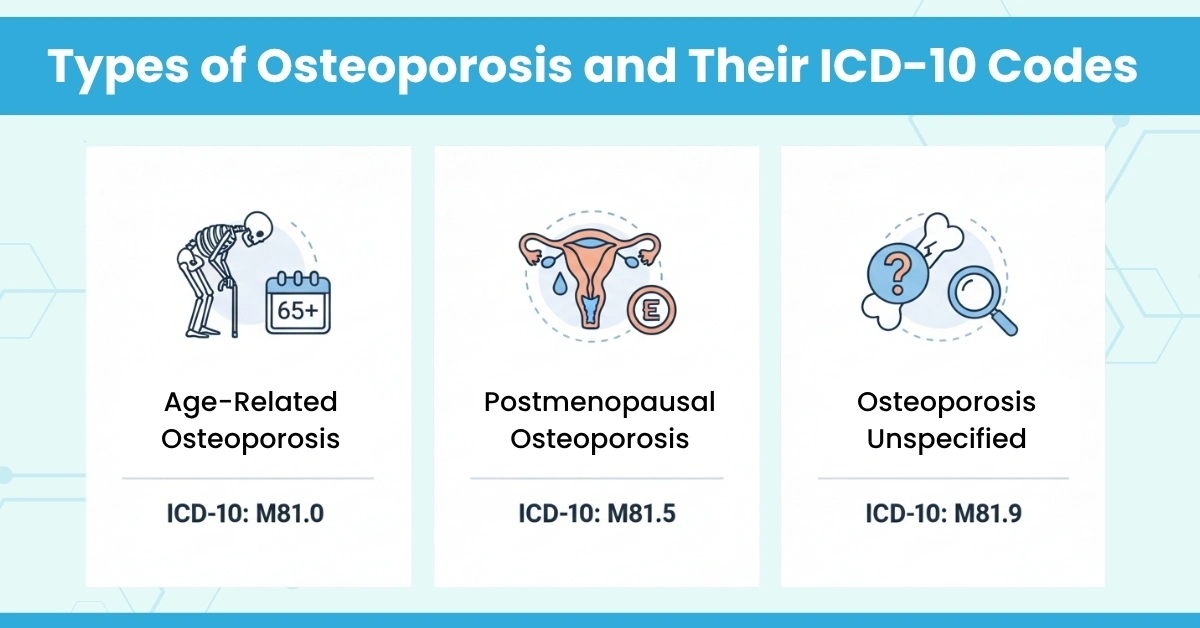
Let’s break down three important subtypes of osteoporosis and how to code them correctly.
Often encountered in older adults, the term “age-related osteoporosis ICD-10” covers cases where bone density loss is largely due to aging/senescence, and there is no current pathological fracture.
Documentation Tip: Clearly mention “without current pathological fracture” and any past fractures as history (with Z87.310) when applicable.
Explicitly identifying postmenopausal osteoporosis can improve coding accuracy:
Because many practices just code “osteoporosis” generically, explicitly identifying “postmenopausal” etiology can support more accurate coding and billing.
When documentation lacks specific detail (etiology unclear, fracture status unknown), the term “osteoporosis unspecified ICD-10” or “unspecified osteoporosis ICD-10” becomes applicable.
But the use of these unspecified codes should be limited. they often trigger audits from payers or internal compliance teams. Good documentation through Hello MD’s medical coding services helps minimise the need for “unspecified” codes.
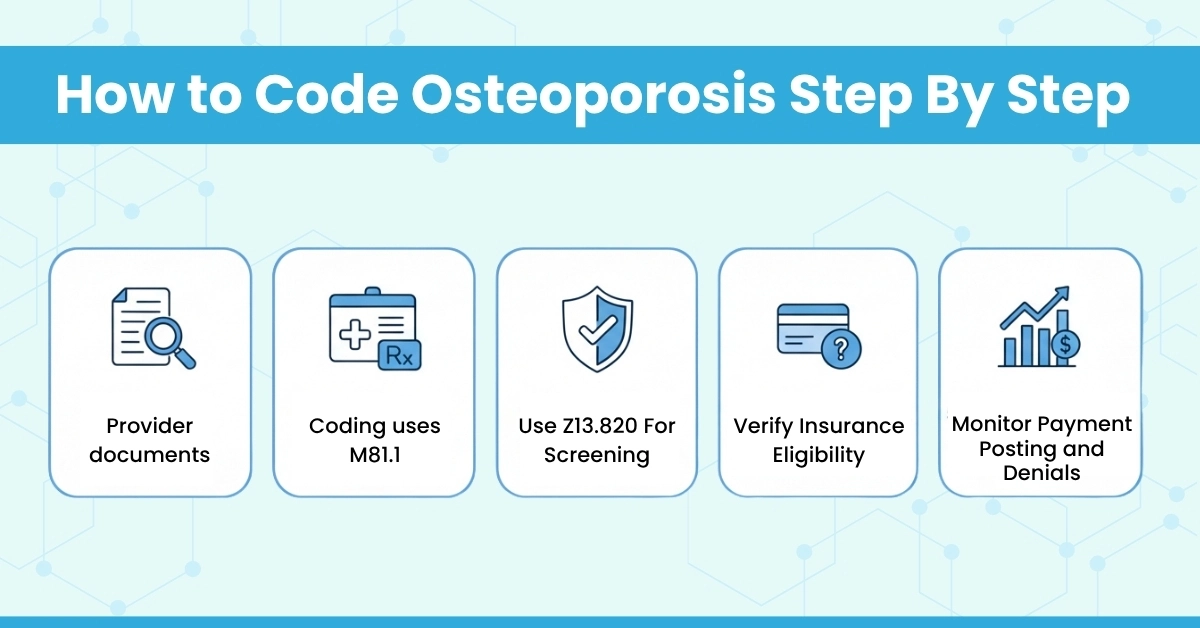
Another area many miss: screening vs diagnosis. The term “ICD-10 code for osteoporosis screening” points to preventive care encounters (e.g., bone density scan/DXA) rather than a confirmed diagnosis.
When a healthy (or asymptomatic) patient undergoes bone density screening, this Z-code is appropriate.
It’s essential to distinguish this from a diagnosis code: If osteoporosis is diagnosed during the visit, you transition to M80/M81 rather than a Z-code. Correct coding supports proper billing, avoids claim denials, and aligns with platforms like HelloMDs’ denial management and billing oversight services.
Let’s walk through a workflow that links clinical documentation, coding, billing, and how Hello MDs integrates:
Scenario: A 72-year-old female patient presents for routine care. A DXA scan shows T-score -2.8 (osteoporosis). No current fracture.
Coders then move to M80.052A (left femur, initial encounter), and HelloMDs’ denial management team monitors for potential payor scrutiny.
This kind of integrated workflow, clinical, coding, billing, and revenue cycle, reflects how HelloMDs adds value. It also shows how catching the right code early (M81 vs M80) influences cost and reimbursement.
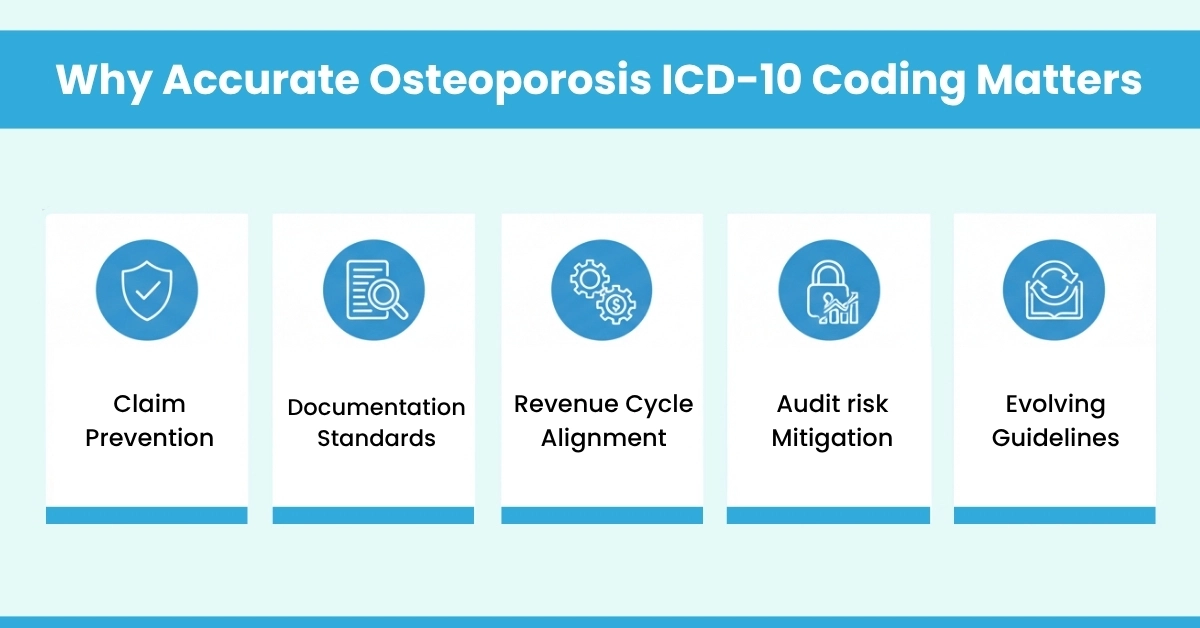
Understanding osteoporosis ICD-10 codes isn’t just about choosing between M80 and M81. It’s about knowing when it’s for screening or diagnosis, whether there’s a fracture or not. How each detail ties back to smooth revenue management. If your office works with Hello MDS, accurate coding means cleaner claims, fewer denials, faster payments, and less stress. Keep this guide handy, fine-tune your process, and let your billing team stay compliant while you stay focused on patient care
This blog is intended for learning and reference, not as a substitute for professional medical or billing advice. Confirm all codes with official ICD-10 resources. Images are AI-generated to support understanding.