Accuracy in medical coding is more than just a formality; it is essential for proper documentation, billing, compliance, and maintaining revenue flow. Hyperlipidemia is one of the most prevalent conditions in medical practice, particularly in internal medicine, family medicine, and cardiology practices.
Hyperlipidemia, also known as dyslipidemia or high cholesterol, is not only a health issue but also a billing and coding problem when not recorded properly. ICD-10 code for Hyperlipidemia (E78.5) is common throughout the U.S.; numerous practices are getting claims denied due to the lack of specificity in the coding process.
In this guide, we will explain hyperlipidemia ICD-10 codes, documentation, medical billing processes, credentialing, payer-related specifications, and prevent expensive denials.
What is Hyperlipidemia?
Hyperlipidemia is a metabolic condition in which an excessive amount of fat is present in the body, such as cholesterol or triglycerides. It is common that most patients do not have the symptoms at first. If a patient doesn’t treat the hyperlipidemia, this causes atherosclerosis, cardiovascular disease, and stroke.
Causes of Hyperlipidemia
- Family history (genetic/familial hypercholesterolemia)
- Consuming excessive amounts of dietary oils and fats.
- Lack of exercise
- Being overweight or obese
- Medical conditions like diabetes and hypothyroidism
- Some medications can also raise cholesterol levels
Symptoms of Hyperlipidemia
- Usually, none at first
- Small fatty deposits under the skin called xanthomas
- Rarely fatigue or chest pain if heart issues develop
- Diagnosis is mostly via blood tests called a lipid panel
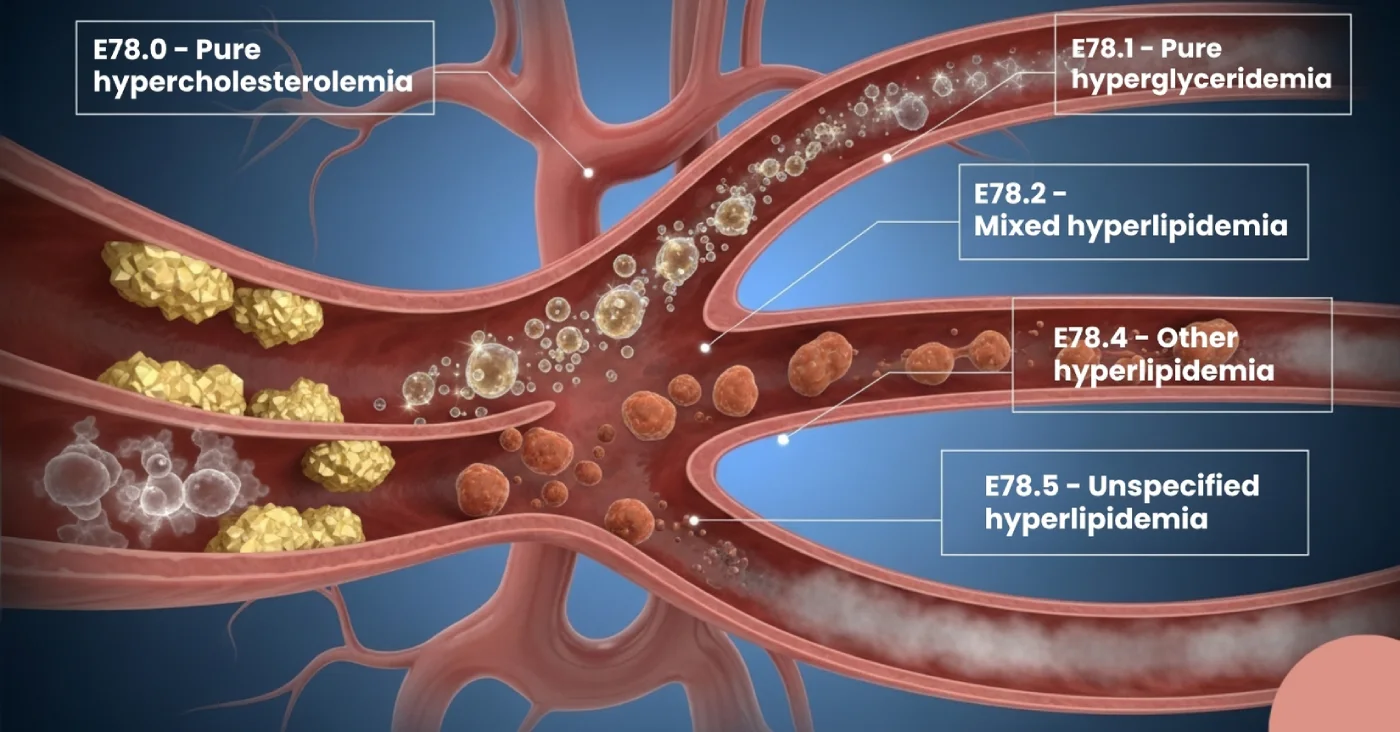
ICD-10 Codes for Hyperlipidemia and Their Meanings
- E78.0 – Pure hypercholesterolemia: Elevated cholesterol only.
- E78.01 – Familial hypercholesterolemia: Genetic disorder with very high cholesterol.
- E78.1 – Pure hyperglyceridemia: Elevated triglycerides.
- E78.2 – Mixed hyperlipidemia: Combination of cholesterol and triglycerides.
- E78.4 – Other hyperlipidemia: Other specified types.
- E78.5 – Unspecified hyperlipidemia: Used when the provider doesn’t specify the type.
Pro Tip for Coders: Always encourage providers to document the type of hyperlipidemia instead of defaulting to unspecified (E78.5). Specific coding improves payer acceptance and helps practices avoid claim audits.
Why Accurate ICD-10 Coding for Hyperlipidemia Matters
The ICD-10-CM coding system places hyperlipidemia under Chapter 4: Endocrine, Nutritional, and Metabolic Diseases.
- E78.5-Hyperlipidemia, unspecified, is the most frequently used code but is often flagged by payers if overused.
- E78.2-Mixed hyperlipidemia is another common code since many patients present with both cholesterol and triglyceride elevations.
- For hereditary cases, E78.01-Familial hypercholesterolemia ensures precise documentation.
Why Accurate ICD-10 Coding Essential
- Support medical necessity for lab testing.
- Justify E/M visit levels.
- Avoid payer denials and audits.
- Ensure proper risk adjustment and chronic care management.
Why it matters in billing:
- Incorrect or non-specific coding can result in claim denials, delays, and reduced reimbursement.
- For value-based care models, accurate coding supports risk adjustment and ensures providers are reimbursed fairly for managing chronic conditions.
Medical Billing and Coding for Hyperlipidemia
For medical billers and coders, hyperlipidemia coding directly impacts revenue cycle performance. Here’s how:
1. Common CPT and ICD-10 Code Combinations
- 80061-Lipid Panel (CPT) paired with E78.x (ICD-10).
- CPT codes for office visits (99213, 99214) often use hyperlipidemia as the primary diagnosis.
2. Billing Challenges
- Overuse of E78.5 may trigger payer denials.
- Missing linkage between hyperlipidemia and comorbidities (e.g., diabetes, obesity).
- Lack of medical necessity documentation.
3. RCM (Revenue Cycle Management) Impact
- Accurate coding leads to clean claims and faster payments.
- Poor documentation of denials, appeals, and lost revenue.
- Coding precision helps avoid payer audits and compliance risks.
Best Practices for Clinical Documentation
To ensure that claims for hyperlipidemia are paid without issues, providers should follow strong clinical documentation improvement (CDI) practices. Repeated use of E78.5 without lab specificity is a top reason for lab claim denials, particularly under Medicare Advantage and commercial plans.
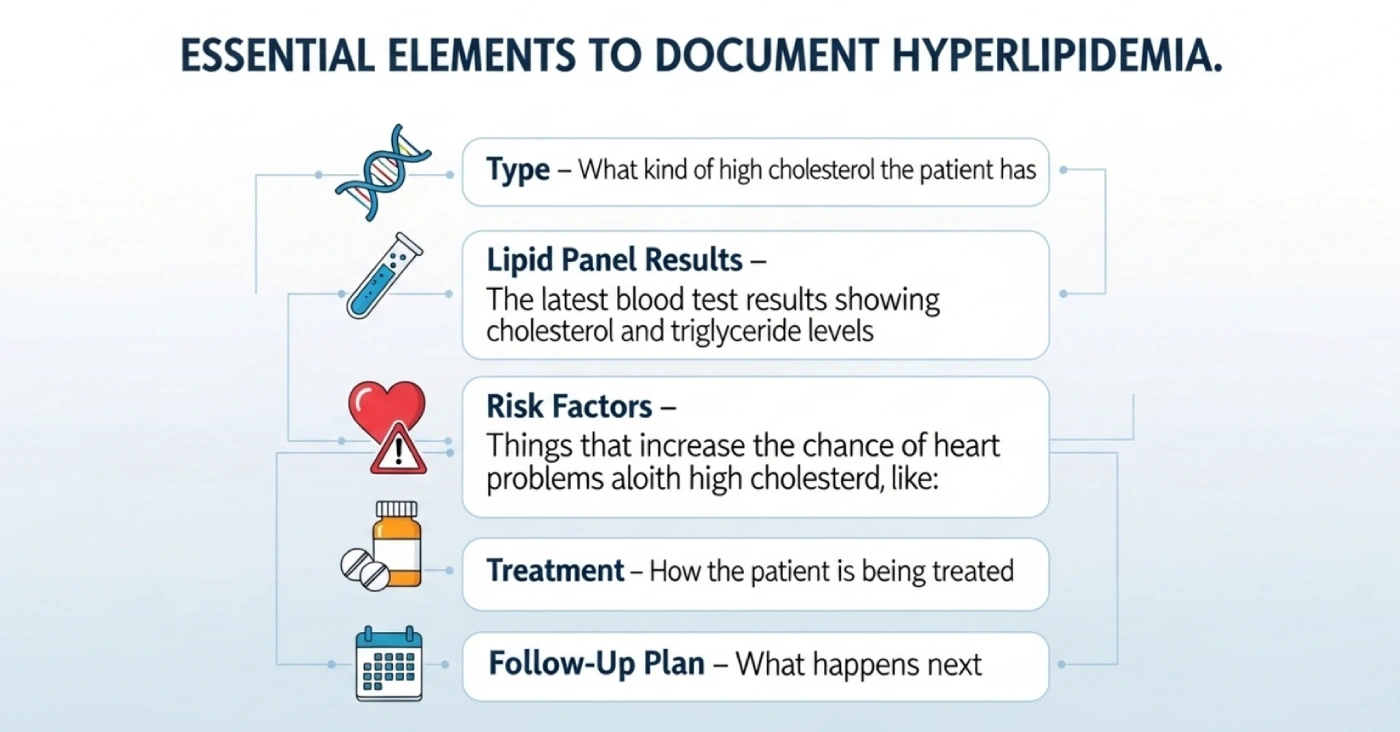
Essential Elements to Document Hyperlipidemia
- Type: What kind of high cholesterol does the patient have? Pure, mixed, familial, or unspecified.
- Lipid Panels: The latest blood test results showing cholesterol and triglyceride levels.
- Risk factors: Things that increase the chance of heart problems, along with high cholesterol, like Diabetes, obesity, smoking, and hypertension.
- Treatment: How the patient is being treated, like Medications (statins, fibrates, niacin) or lifestyle modifications.
- Follow-up plan: What happens next? When the next cholesterol (lipid panel) test will be done, how the patient’s progress will be monitored, and what long-term management steps are planned.
Example of weak documentation:
“Patient has high cholesterol.” (Not specific enough for coding).
Example of strong documentation:
“Patient diagnosed with mixed hyperlipidemia (E78.2). LDL: 160 mg/dL, triglycerides: 250 mg/dL. Started atorvastatin, advised dietary changes, follow-up in 3 months.”
Strong documentation gives coding accuracy, payer compliance, and also reduces denials.
Credentialing and Payer Considerations
Even the best coding won’t help if the provider is not credentialed with the payer. Credentialing ensures the provider is authorised to bill Medicare, Medicaid, or commercial insurance.
Importance of Credentialing in Hyperlipidemia Claims:
- Payers demand that providers enrol and credential providers to process claims.
- Credentialing assists in determining eligibility for reimbursement of CPT 80061 and follow-up visits.
- Payer-specific conditions (Medicare vs. private insurance) might be different with regard to lipid testing coverage.
Example: Medicare can provide lipid panels on an annual basis to patients who have cardiovascular risk factors, but commercial insurers can offer them more often in accordance with the clinical need.
In the case of clinics and solo practitioners, outsourcing medical billing and credentialing can be an effective solution to have claims of hyperlipidemia and other chronic conditions approved within a short duration without the administrative hassle.
Related Conditions & Additional Coding Tips
Hyperlipidemia often does not exist in isolation; it’s commonly linked to other chronic diseases. Coding these correctly improves risk adjustment scoring and supports medical necessity.
Common Comorbid Conditions:
- Diabetes Mellitus (E11.9): often coded alongside hyperlipidemia.
- Obesity (E66.9) – major risk factor.
- Hypertension (I10): frequently present with lipid disorders.
- Hypothyroidism (E03.9): can cause secondary hyperlipidemia.
- Atherosclerosis (I70.x): progression due to lipid buildup.
Coding Scenarios Tips That Help
- Scenario 1: For Patient with elevated LDL only → E78.0 – Pure hypercholesterolemia.
- Scenario 2: For Diabetic patient with elevated LDL and triglycerides → E78.2 – Mixed hyperlipidemia + diabetes ICD-10.
- Scenario 3: For New diagnosis awaiting lab confirmation → E78.5 (temporary use only).
- Scenario 4: For Statin follow-up visit → Specific hyperlipidemia ICD-10 + appropriate E/M code.
The Audit Risk: Why Correct Coding Matters
Insurance companies and CMS conduct audits to detect upcoding, undercoding, or misuse of unspecified codes. Overusing E78.5 can be a red flag.
- Undercoding: Using unspecified codes when more detail exists → leads to lost revenue.
- Overcoding: Using higher complexity codes without supporting documentation → can trigger penalties.
Maintaining compliance protects your practice from denials, takebacks, and legal issues.
Conclusion
What appears to be a very straightforward code, hyperlipidemia (ICD-10 code E78.5), has a significant impact on medical billing and credentialing. Clean claims, fewer denials, and stable performance of the revenue cycle can be achieved through proper documentation, coding to specificity, and payer compliance.
Hello MDs assists medical facilities in medical billing, credentialing, and revenue cycle management (RCM). Our experts help ensure accurate coding, payer compliance, and faster reimbursement, so your team can focus on delivering high-quality patient care.